

Raba Thapa,1 Sanduk Ruit,1 Paul S Bernstein2 1
Tilganga Institute of Ophthalmology, Kathmandu, Nepal, 2Moran Eye Center, University of Utah, USA.
ABSTRACT
Background: This study aimed to assess skin carotenoid measurement among children in the Hill region of Nepal. Methods: School children between 3 to 7 years old from six schools were enrolled in the study. Skin carotenoid levels were assessed using the Veggie Meter® (Longevity Link Corporation, Salt Lake City, Utah, USA). Detailed eye evaluations were conducted in subjects with low skin carotenoid scores (<150 Reflectance Units (RU)) and/or those with a history of night blindness.
Results: A total of 324 school children were enrolled in the study with mean age of 5.12±1.33 years. The mean skin carotenoid score was 163±71 RU, ranging from 1 to 363 RU. The skin carotenoid level was <150 RU in 46.9% of children and between 150 and 200 RU in 23.5% of children. Low skin carotenoid scores (<150 RU) were found in 17% of 3-year-olds, 28.3% each of 4- and 5-year-olds, 20.4% of 6-year-olds, and 11.2% of 7-year-olds. In multivariate analysis, age was significantly associated with low skin carotenoid scores (p=0.003; OR; 2.02; 95% CI: 1.28- 3.19). Odds of having <150 RU was 2.02 times more among the children up to five years old as compared to those over five years of age.
Conclusions: Nearly half of the school children had low skin carotenoid scores. Skin carotenoid score was significantly lower among the lower age group. These findings emphasize the need to enhance awareness to consume plenty of green leafy vegetables and fruits in the diet. Keywords: Children; Nepal; skin carotenoid; veggie meter; vitamin A.
INTRODUCTION
Carotenoids such as beta-carotene are the major dietary source of vitamin A. Low levels of carotenoid intake could lead to vitamin A deficiency (VAD), especially among high-risk people like children.1,2 VAD is a public health problem in many low- and middle-income countries including in Nepal.3-6 VAD is usually assessed by measuring serum retinol, but this test is not available in many developing countries such as Nepal. Skin carotenoid measurement using non-invasive devices could be utilized as a rapid screening tool for adequate consumption of green leafy vegetables and fruits.7,8 Recently, we have shown that the Veggie Meter®, a portable device that uses reflection spectroscopy to measure skin carotenoid levels8, can be used to screen skin carotenoid levels as a biomarker for VAD in outlying regions of Nepal.9 Since there is limited information about skin carotenoid levels among high-risk groups for VAD in Nepal, this study aimed to assess the skin carotenoid score among school children three years to seven years of age in the Hill region of Nepal.
METHODS
A cross-sectional study was conducted among school children from three years to seven years of age in the Nuwakot district, a Hill region of Nepal. Children were enrolled from six schools: five public and one private.
Based on the 49% prevalence of low skin carotenoid levels (<150 Refection Unit (RU)) among children of 8 to 12 years of age in a previous study in the Hill region,9 the minimum sample size was 294. Assuming 10% non-response, the total sample size for the study was 324. An equal number of children were selected from each school using a random sampling method (Lottery method).
Children aged 3 years to 7 years were eligible for the study. The prior study conducted among the 8 years to 12 years of age at the same study area showed high prevalence of low skin carotenoid. So, this study was conducted to enroll the other age groups child from the same study area.
Children were excluded from the study if their parent or guardian did not provide written informed consent to enroll in the study. Children whose fingers on both hands had scars or abnormal staining despite thorough hand washing were excluded from the study.
Ethical approval was obtained from the Nepal Health Research Council to conduct the study (Reference no. 1079/2021). The study adhered strictly to the tenets of the Declaration of Helsinki. Parents or local authorized guardians provided informed consent for the children before enrollment in the study.
Demographic details of study participants taken were age, gender, occupation, educational level, height and weight for body mass index (BMI) calculation, dietary history (whether a vegetarian or not, and frequency of vegetables and fruit ingestion), and use of vitamin A supplements. Information regarding any history of ocular or systemic problems was collected. Height and weight of the study participants were recorded during the data collection. BMI was calculated using the formula BMI= Weight in KG/Height in meter.
Visual acuity assessment was done as a part of ocular examination for all children. Uncorrected visual acuity, and best corrected visual acuity using the pin hole was recorded for all children enrolled in the study. Visual impairment was classified as per the WHO criteria. Those with the visual acuity of 6/9 or worse were referred to the nearby district community eye center for the refraction and glasses as needed.
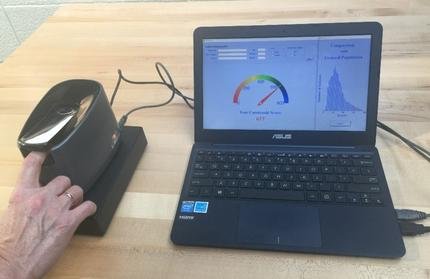
The Veggie Meter® produced by Longevity Link Corporation, Salt Lake City, UT, USA, was used in this study to assess skin carotenoid status by pressure-mediated reflectometry.8 Picture of Veggie Meter has been shown in Figure 1. It is a validated, rapid, non-invasive, and portable device to assess fruit and vegetable intake, and its skin carotenoid score has a strong positive significant correlation with skin resonance Raman spectroscopy and total serum carotenoids.8,9 In brief, finger preferably index finger is illuminated with broad-band white light spanning the spectral range from 350-850 nm, and the spectral composition of the diffusively reflected light is analyzed in real-time. A participant gently presses their index finger against the convex lens surface with the help of a spring-loaded cover, which momentarily squeezes blood out of the illuminated tissue volume, reducing oxy-hemoglobin and other chromophores’ influence on the reflection spectra. 9 A laptop computer connected to the Veggie Meter® regulates the light exposure, data acquisition, processing, and display of the reflection spectra. The display provides the skin carotenoid score on a scale from 0 to 800 RU. In this study, the single scan mode lasting about 10 seconds was used. Three single readings were collected from the same finger, and the average score was taken as the final skin carotenoid score. Participants had their hands sanitized or washed before each measurement, and the device was calibrated daily with the dark and white reference sticks before starting measurements and at least every two hours when doing multiple skin measurements over long periods.9
Those children having skin carotenoid scores <150 RU or with a history of night blindness had a comprehensive ocular assessment under mydriasis using slit-lamp bio microscopy, and direct or indirect ophthalmoscopy.
Figure 1. Veggie Meter.
Data were entered into MS Excel. Data cleaning and coding were also done in MS Excel. Data were transferred to Statistical Package for the Social Sciences (SPSS) V20 developed by IBM for statistical analysis. For categorical data analysis, Chi square and Fisher Exact tests were used wherever applicable. For continuous variables, independent t-tests or Mann Whitney U-tests were used for normally distributed and non-normally distributed data, respectively. All significant variables found in bivariate analysis were taken for binary logistic regression to quantify the results. P values <0.05 were considered statistically significant.
RESULTS A total of 324 study participants were enrolled from six schools, five public and one private. Fifty-four students (16.7%) each were enrolled from four schools. There were only 51 eligible participants in one of the public schools, so 57 participants were enrolled from a subsequent public school.
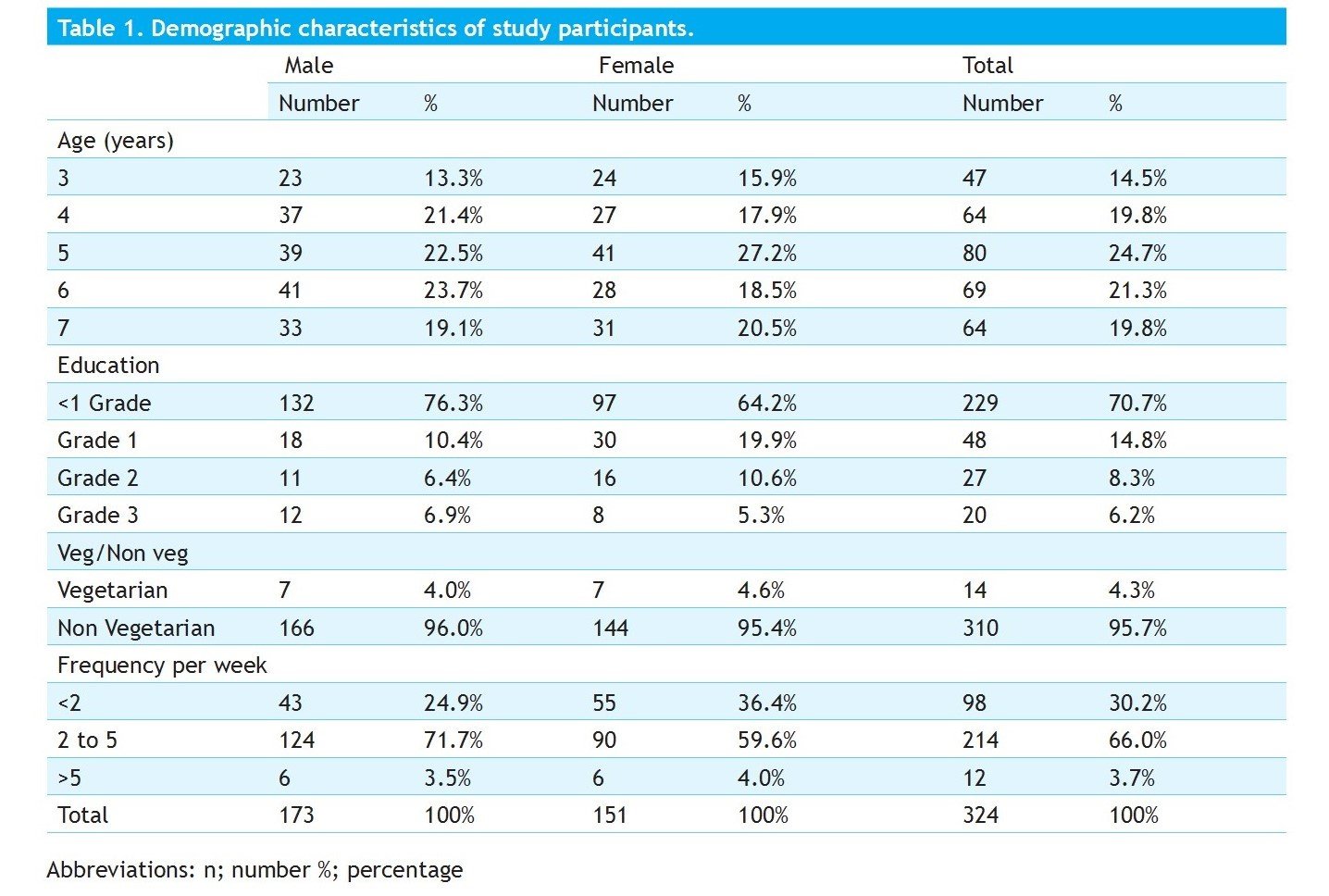
The mean age of children enrolled in the study was 5.12 ± 1.33 years, with age ranging from 3 to 7 years. Among the enrolled children, the majority of children were 5 years of age (24.7%) and lowest in number at 3 years of age (14.5%). Males were slightly higher in number (53.5%) as compared to females (46.5%). The majority of children were studying below grade one at 229 subjects (70.7%). A total of 14 children (4.3%) were pure vegetarian. 214 children (66%) had a history of consumption of green leafy vegetables 2 to 5 times per week (Table 1).
Among the study participants, six (1.85%) had ocular complaints and two (0.61%) had systemic complaints. The systemic complaints were itching in ears and cough (one case each). Blurring of vision was the most common ocular complaint, with five cases (1.54%) among the study participants (Table 2)
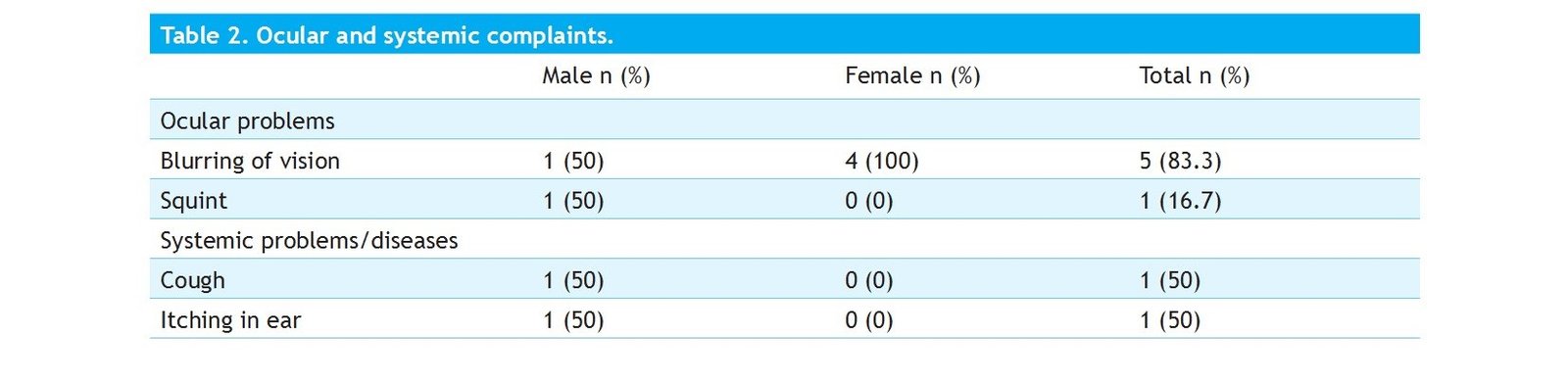
Ocular problems Blurring of vision, Squint Systemic problems/diseases, Cough, Itching in ear
Assessment of Skin Carotenoids among School Children
The mean skin carotenoid score was 163 ±7 RU, ranging from 1 to 363 RU. The mean skin carotenoid score among the children between 3 to up to 5 years of age was 150 ±69 RU, ranging from 1 to 363 RU. The mean skin carotenoid score of children over five years up to seven years was 181 ± 70 RU, ranging from 1 to 341 RU.
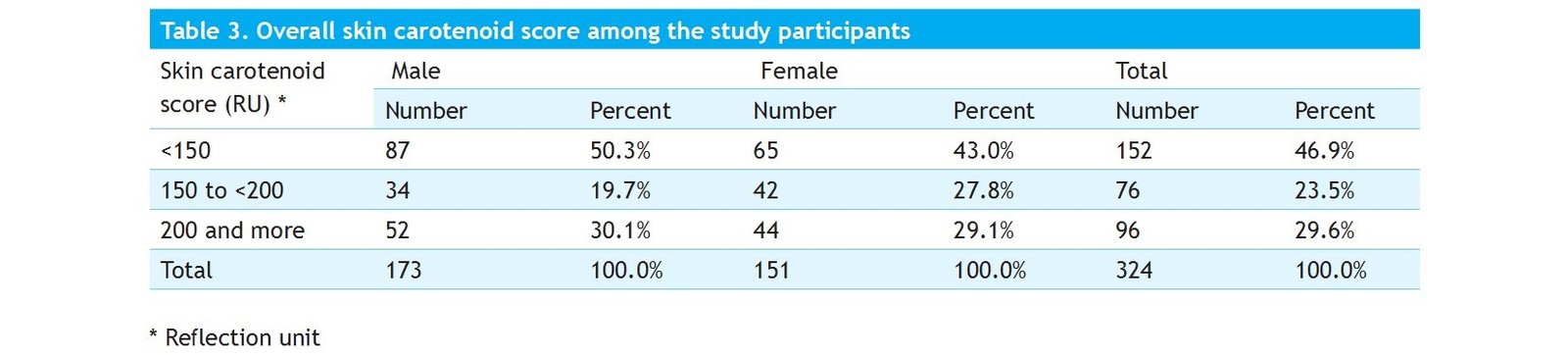
The skin carotenoid level was < 150 RU in 152 participants (46.9%) of children, between 150 and 200 RU in 76 participants (23.5%), and >200 RU in 96 participants (29.6%).
Skin carotenoid scores less than 150 RU were found in 87 male subjects (50.3%), whereas among the females, 65 (43%) had skin carotenoid levels less than 150 RU. (Table 3).
Among the children of various schools, the prevalence of skin carotenoids score less than 150 RU ranged from 9.8% to 74.1%. Skin carotenoid scores of 150 to <200 ranged from 11.1% to 33.3%.
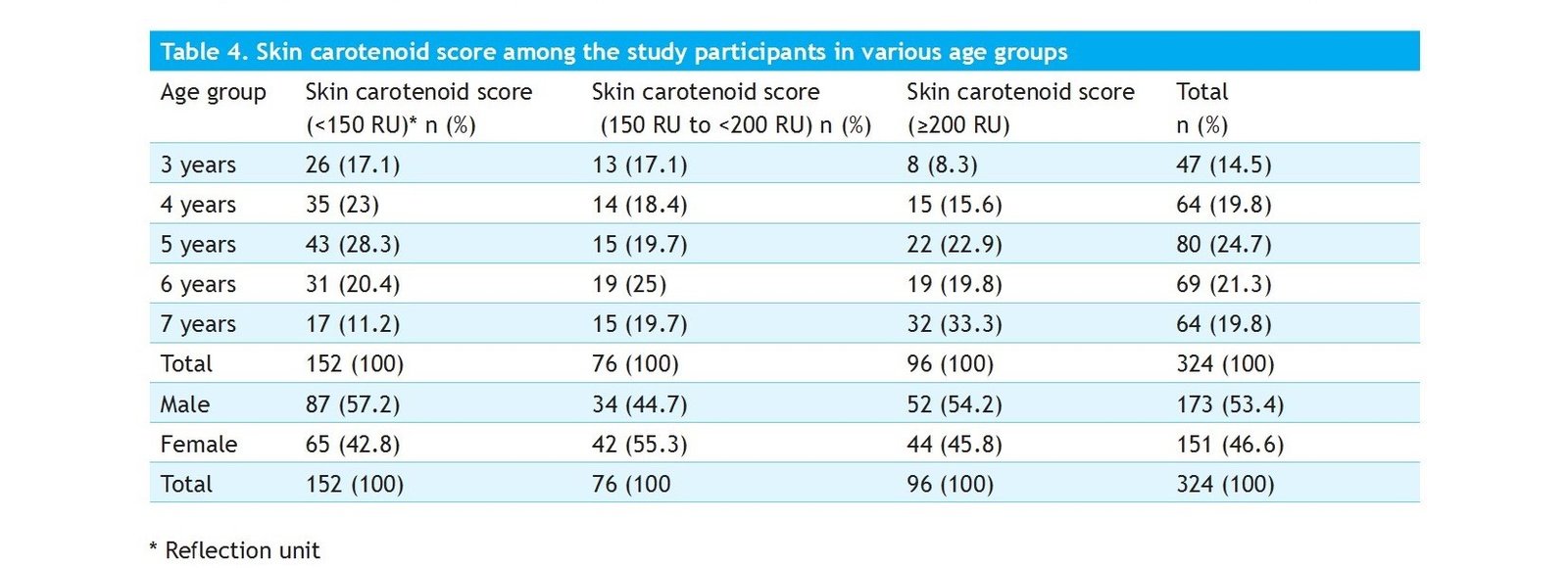
Low skin carotenoid (<150 RU) was found in 26 cases (17%) at 3 years of age, 35 cases (28.3%) at 4 years of age, 43 cases (28.3%) at 5 years of age, 31 cases (20.4%) at 6 years of age, and 17 cases (11.2%) at 7 years of age. (Table 4)
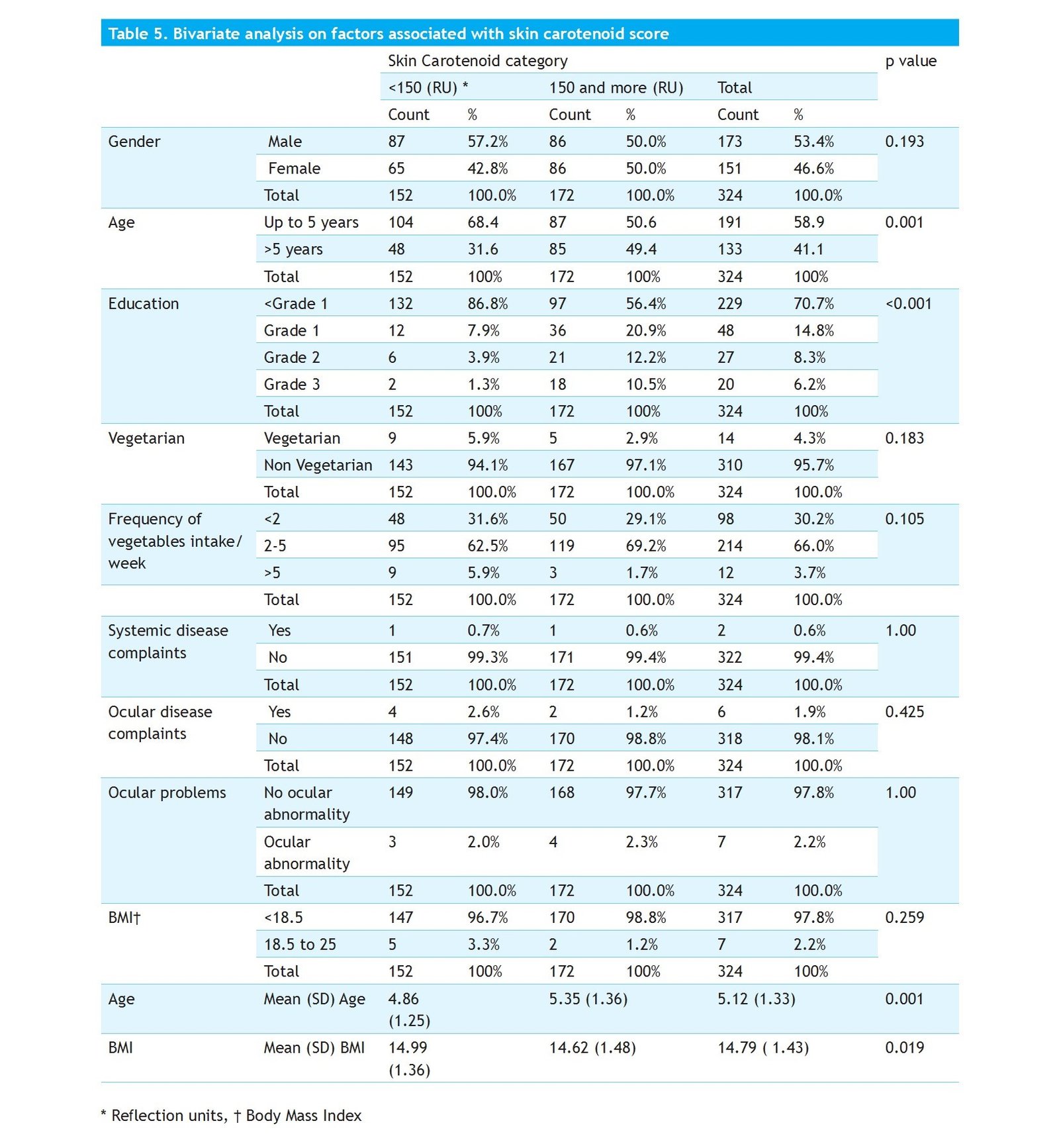
Among the various variables in bivariate analysis, there was significant association of low skin carotenoid with age (p=0.001) and BMI (p=0.019). Gender associations were not statistically significant with skin carotenoid category. (Table 5).
None of the children had a history of night blindness or signs of xerophthalmia among the participants with low skin carotenoids or normal carotenoids. The other ocular morbidities noted were refractive error with uncorrected visual acuity of less than 6/12 in 6 cases (1.9%) and allergic conjunctivitis in one case (0.3%). Those with the visual acuity of 6/9 or worse were referred to the nearby district community eye center for the refraction and glasses as needed.
DISCUSSION
Our study assessed the skin carotenoid score among school going children aged 3 to 7 years in the Hill region of Nepal. Vitamin A is obtained from two major sources: preformed vitamin A, retinol, and pro-vitamin A carotenes, some of which are converted to retinol, a process that takes place in the human gut and elsewhere. Pro-vitamin A carotenoids are found in abundant quantities in green leafy vegetables and fruits such as spinach, amaranth, papaya, mango and pumpkin, etc.2
There are numerous species of dietary carotenoids, and beta-carotene is the major one which is converted to retinol. Carotenoids can be measured individually in serum by HPLC or they can be assessed optically in aggregate in the skin by reflection spectroscopy. This method quantifies all chromophores in the skin and reflects the composite score for all carotenoid species absorbing in the 480 nm range. The carotenoids responsible in this range include α- and β-carotenes, β-cryptoxanthin, lycopene, lutein, and zeaxanthin.8,10 Based on a previous study that we conducted in Nepal, a high carotenoid score in a healthy individual is indicative of a high likelihood of adequate vitamin A status.
The Veggie Meter®, a portable, noninvasive optical device used to measure skin carotenoid scores in our study, found 46.9% of school-going children had skin carotenoid scores below 150 RU, a level possibly associated with a high-risk of VAD. Only 29% of children had skin carotenoid scores >200 RU which is considered to be a normal value.8 This finding was similar to the prevalence of low skin carotenoids (49%) of the 8-to-12-year age group from the same area. This likely reflects the paucity of foods rich in carotenoids in this Hill region. By contrast, a study conducted in hospital settings in Japan and Utah reported average skin carotenoid score of 335 RU and 297 RU, respectively.8 The mean skin carotenoid score among the children was 163 ± 71 RU, ranging from 1 to 363 RU. A California study conducted among 1000 daycare children ages two to five years reported an average score of 380 RU. The skin carotenoid score of our children was much lower than this study.8
The low skin carotenoid score was very high up to the age group 5 years (68.4%) as compared to above five years of age (31.6%). The skin carotenoid score of children will not be affected by the vitamin A supplementation. So, the lower skin carotenoid score is related to the inadequate intake of green leafy vegetables and fruits. This could also be due to consumption of the overcooked green leafy vegetables that destroys the carotenoids among our children.
Among the children of various schools, the prevalence of skin carotenoids score less than 150 RU ranged from 9.8% to 74.1%. A low prevalence of skin carotenoid scores <150 RU was found in relatively remote schools, where the inhabitants largely consume vegetables from their own garden and fish from nearby rivers. A high prevalence of skin carotenoid score <150 RU was found among schools situated in urban areas with rare family gardens, where they are more likely to consume carotenoid-poor biscuits and noodles. Studies conducted in children aged 5 to 17 years show a significant positive correlation of skin carotenoid with serum carotenoids,11 and skin carotenoid levels can be used as a biomarker of fruit and vegetable intake.11-13
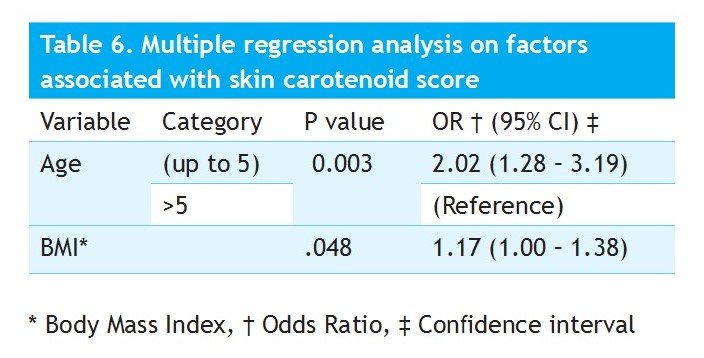
Low skin carotenoid scores (<150 RU) were found maximally in the age four- and five-years groups, comprising of 28.3% each and were lowest at the age of seven years comprising of 11.2%. Similarly in multivariate analysis, age was significantly associated (p=0.003) with a low skin carotenoid score where the odds of having <150 RU was 2.02 times more among the children up to five years as compared to those over five years of age. This could be due to inadequate consumption of green leafy vegetables by small children.
Education of parents to encourage more consumption
of green leafy vegetables and fruits by their children could help improve skin carotenoid levels. Emphasis on awareness and education of vitamin A and its dietary source to school teachers and serving of plenty of green leafy vegetables and fruits in mid -day school lunch programs could help raise skin carotenoid scores.
The government program of vitamin A supplementation from six months to five years for children throughout the nation in Nepal seems effective in reducing VAD sequelae among these small children. Despite the high prevalence of low skin carotenoids, we did not find any children with features of xerophthalmia. Based on the findings of this study, we recommend the continued use of Vitamin A supplementation among these children until five years of age and education regarding increased consumption of green leafy vegetables and fruits in their diet.
The strength of our study is its large sample size selected randomly from various public and private schools. On the other hand, our participants were enrolled from a single district, so our findings cannot be generalized to other geographical areas of the Hill region. Further studies are recommended involving larger, more diverse geographical areas in varied seasons of the year.
CONCLUSIONS
Nearly half of the school children participating in this study had low skin carotenoid scores (<150 RU), levels highly suggestive of VAD. Skin carotenoid score was significantly lower among the younger age group. In addition to enhancing awareness to increase consumption of green leafy vegetables and fruits, vitamin A supplementation should be continued to combat vitamin A deficiency in children in the Hill region of Nepal.
ACKNOWLEDGEMENTS
Thrasher Research Fund: Early Career Research Award Grant 2020 for conduction of this study. Moran Eye Center, University of Utah, USA: for Veggie Meter support free of cost to the research project. Tilganga Institute of Ophthalmology: Kathmandu, Nepal for technical and logistic supports. The study was presented at the 2nd Virtual International Carotenoid Society Conference, April 12-14, 2022.
CONFLICT OF INTEREST None of the authors have any conflict of interest.
REFERENCES
- Blaner WS. Vitamin A and provitamin A carotenoids. Present Knowledge in Nutrition: Elsevier; 2020. p. 73-91.doi:
https://doi.org/10.1016/B978-0-32366162-1.00005-6
- Carazo A, Macáková K, Matoušová K, Krčmová LK, Protti M, Mladěnka P. Vitamin A Update: Forms, Sources, Kinetics, Detection, Function, Deficiency, Therapeutic Use and Toxicity. Nutrients. 2021;13(5). doi: https://doi.org/10.3390/nu13051703
- Akhtar S, Ahmed A, Randhawa MA, Atukorala S, Arlappa N, Ismail T, et al. Prevalence of vitamin A deficiency in South Asia: causes, outcomes, and possible remedies. J
Health Popul Nutr.
2013;31(4): 413-23.doi: jhpn. v31i4.19975
https://doi.org/10.3329/
- World Health Organization. Global prevalence of vitamin A deficiency in populations at risk 1995-2005: WHO global database on vitamin A deficiency. 2009.
- Micronutrient Initiative, Ministry of Health and Population (Nepal), National Planning Commission (Nepal), New ERA, United Nations Children’s Fund (UNICEF), World Health Organization (WHO). Nepal Micronutrient Status Survey. Nepal National Micronutrient Status Survey, 2016. Kathmandu: Ministry of Health and Population. 2018.
- Micronutrient Initiative, Ministry of Health and Population (Nepal), National Planning Commission (Nepal), New ERA, United Nations Children’s Fund (UNICEF), World Health Organization (WHO). Nepal Micronutrient Status Survey 1997-1998.
- Mayne ST, Cartmel B, Scarmo S, Jahns L, Ermakov IV, Gellermann W. Resonance Raman spectroscopic evaluation of skin carotenoids as a biomarker of carotenoid status for human studies. Archives of biochemistry and biophysics. 2013;539(2):163-70. doi: https://doi.org/10.1016/j.abb.2013.06.007
- Ermakov IV, Whigham LD, Redelfs AH, Jahns L, Stookey J, Bernstein PS, et al. Skin Carotenoids as Biomarker for Vegetable and Fruit Intake: Validation of the Reflection-Spectroscopy Based “Veggie Meter”. The FASEB Journal. 2016;30 (S1): 409.3-.3.doi: https:// doi.org/10.1096/fasebj.30.1_supplement.409.3
- Thapa R, Ruit S, Add Carotenoid Assessment to Detect Vitamin A
Deficiency in Children and Pregnant Women in Nepal. Investigative Ophthalmology & Visual Science. 2022 Jun 1;63(7):2631. doi: https://doi.org/10.1016/j. tjnut.2023.02.005
- Radtke MD, Poe M, Stookey J, Jilcott Pitts S, Moran NE, Landry MJ, et al. Recommendations for the Use of the Veggie Meter® for Spectroscopy-Based Skin Carotenoid Measurements in the Research Setting. Current developments in nutrition. 2021;5(8): nzab104.doi:
https://doi.org/10.1093/ cdn/nzab104
- Aguilar SS, Wengreen HJ, Lefevre M, Madden GJ, Gast J. Skin carotenoids: a biomarker of fruit and vegetable intake in children. J. of the Acad. of Nutr. and Diet. 1142014; :1174–1180.doi: https://doi. org/10.1016/j.jand.2014.04.026
- Jahns L, Johnson LK, Mayne ST, Cartmel B, Picklo Sr MJ, Ermakov IV, et al. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: uptake and depletion kinetics. The American journal of clinical nutrition. 2014;100(3): 930-7.doi:
https://doi.org/10.3945/ ajcn.114.086900
- Conrady CD, Bell JP, Besch BM, Gorusupudi A, Farnsworth K, Ermakov I, et al. Correlations between macular, skin, and serum carotenoids. Investigative ophthalmology & visual science. 2017 Jul 1;58(9): 3616-27.doi: https://doi.org/10.1167/ iovs.17-21818o EK, Bernstein PS. Skin
Correspondence: Dr Raba Thapa, Tilganga Institute of Ophthalmology, Kathmandu, Nepal, Email: rabathap@live.com
Original Article: Journal of Nepal Health Resource Council 2024 Oct.-Dec.;22


प्रतिक्रिया दिनुहोस्